The Neurobiology of Cassandra Syndrome: Trauma Physiology Explained

Most conversations about “Cassandra Syndrome” stop at words like stress, burnout, or emotional exhaustion.
But those words are too small.
What many partners experience in chronically misattuned relationships is not simply frustration. It is prolonged autonomic activation in the context of attachment disruption. And attachment disruption is one of the most powerful biological stressors in adult life.
If you’re a clinician, coach, or analytically minded partner, this lens matters. Because once we shift from psychology alone to physiology, everything starts to make sense.
Let’s walk through what’s actually happening in the body.
Chronic Emotional Vigilance Is Autonomic Activation
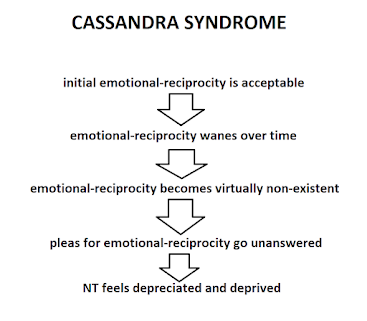
In relational systems where emotional attunement is inconsistent, dismissive, or unpredictable, the nervous system does not stay neutral.
It adapts.
When bids for connection are regularly met with withdrawal, tone shifts, stonewalling, cognitive reframing without empathy, or emotional invalidation, the body does not interpret these as “personality differences.”
It interprets them as attachment instability.
And attachment instability activates survival circuitry.
Here’s the sequence:
The amygdala detects threat.
The amygdala signals the hypothalamus.
The hypothalamus activates the HPA axis (hypothalamic–pituitary–adrenal axis).
This cascade unfolds rapidly:
-
Corticotropin-releasing hormone (CRH)
-
Adrenocorticotropic hormone (ACTH)
-
Cortisol release from the adrenal cortex
Occasional activation resolves. The system returns to baseline.
But when micro-threats accumulate daily — abrupt tone shifts, emotional dismissiveness, unpredictability — baseline cortisol begins to shift upward.
What started as a state becomes a trait.
The partner becomes hypervigilant not because they are “too sensitive,” but because their nervous system has learned that emotional ambiguity equals potential threat.
HPA Axis Dysregulation and Allostatic Load
The body is remarkably adaptive. It uses a process called allostasis — stability through change — to adjust to stressors.
But chronic allostasis becomes wear and tear. This wear and tear is called allostatic load.
In long-term relational stress, we often see:
-
Flattened diurnal cortisol curves
-
Elevated evening cortisol
-
A blunted morning cortisol awakening response
-
Reduced heart rate variability (HRV)
-
Increased sympathetic dominance
Clinically, this shows up as:
-
3 AM waking
-
Non-restorative sleep
-
Brain fog
-
Irritability
-
Reduced stress tolerance
-
Emotional reactivity that feels disproportionate
The system loses flexibility.
And rigidity — not intensity — is the hallmark of trauma physiology.
When the nervous system can no longer move fluidly between activation and recovery, the body pays the price.
A Polyvagal Perspective
From a polyvagal framework, chronic relational misattunement reduces ventral vagal activation — the branch of the vagus nerve responsible for social engagement and felt safety.
The ventral vagal system supports:
-
Facial expressivity
-
Vocal prosody
-
Eye contact
-
Emotional warmth
-
Digestive efficiency
When attunement is unreliable, the system shifts away from ventral vagal regulation and toward survival states:
Sympathetic mobilization (fight/flight)
or
Dorsal vagal withdrawal (shutdown)
Many partners oscillate between both.
Hypervigilant during interaction.
Collapsed after conflict.
This oscillation is metabolically expensive. The body is either bracing or conserving.
Neither state promotes healing.
And over time, the nervous system forgets what sustained safety feels like.
Inflammation and Immune Signaling
Chronic relational stress does not stay in the brain. It reaches the immune system.
Emotional threat activates pro-inflammatory cytokines such as:
-
Interleukin-6 (IL-6)
-
Tumor necrosis factor alpha (TNF-α)
-
C-reactive protein (CRP)
Why?
Because evolution wired social rejection to equal survival threat. In ancestral environments, isolation meant danger.
So the immune system mobilizes.
Over time, elevated inflammatory signaling contributes to:
-
Weight gain
-
Autoimmune vulnerability
-
Gastrointestinal dysregulation
-
Fatigue
-
Increased pain sensitivity
This is not psychosomatic.
It is psychoneuroimmunology.
The body does not distinguish between relational threat and physical threat as cleanly as we like to think.
Metabolic Consequences
Cortisol increases gluconeogenesis — the production of glucose. Chronically elevated glucose leads to increased insulin secretion. Elevated insulin promotes fat storage, particularly visceral fat.
Visceral adiposity then increases inflammatory cytokines.
Now we have a feedback loop:
Emotional stress → Cortisol → Insulin → Visceral fat → Inflammation → Increased stress sensitivity.
This is why “just diet harder” often fails under chronic relational stress.
The metabolic environment is stress-driven.
Until autonomic tone shifts, the body resists fat loss not because of willpower deficits, but because of survival coding.
The body prioritizes safety over aesthetics.
Always.
Attachment Trauma in Adulthood
We often reserve the word trauma for overt abuse.
But chronic emotional invalidation within attachment bonds can create what we might call relational developmental trauma in adulthood.
When bids for connection are repeatedly unmet, the nervous system encodes a somatic belief:
“Connection is unstable.”
That belief is not merely cognitive.
It is embodied.
It alters baseline physiology.
Which is why insight alone does not resolve symptoms. You can intellectually understand attachment dynamics and still wake at 3 AM with your heart racing.
The body must experience safety repeatedly and predictably — not just in the relationship, but internally.
Clinical Implications
For clinicians working with Cassandra-type presentations, physiology must lead.
Interventions might include:
-
Targeting autonomic regulation before cognitive reframing
-
Tracking HRV, sleep quality, and metabolic markers
-
Normalizing physiological symptoms as adaptive responses
-
Reducing relational hypervigilance through boundary stabilization
-
Supporting differentiation without forced detachment
For individuals, the shift is equally important.
Healing is not about winning the emotional argument.
It is about recalibrating autonomic tone.
You are not weak.
You are not overreacting.
Your nervous system has been adapting to chronic ambiguity.
The work is physiological before it is relational.
If this perspective resonated at a deeper level — if something inside you felt understood not emotionally, but biologically — that matters.
Because when the narrative shifts from:
“What’s wrong with me?”
to
“My nervous system adapted to prolonged uncertainty,”
shame decreases.
And regulation becomes possible.
In the next conversation, we’ll translate this physiology into structured recovery steps — practical ways to reduce autonomic load, rebuild ventral vagal tone, and interrupt the inflammatory cascade.
Until then, remember:
Your symptoms make sense.
And biology can heal.
 |
| Mark Hutten, M.A. |
Pick Your Preferred Day/Time
Available Classes with Mark Hutten, M.A.:
==> Cassandra Syndrome Recovery for NT Wives <==
==> Online Workshop for Men with ASD level 1 <==
==> Online Workshop for NT Wives <==
==> Online Workshop for Couples Affected by Autism Spectrum Disorder <==
==> ASD Men's MasterClass: Social-Skills Emotional-Literacy Development <==
Individual Zoom Call:
==> Life-Coaching for Individuals with ASD <==
Downloadable Programs:
==> eBook and Audio Instruction for Neurodiverse Couples <==